Summary of safety profile: Severe reactions, such as shock, may occur very rarely with human albumin solutions. In these cases, the infusion must be stopped and an appropriate treatment must be initiated.
Mild undesirable effects, which may occur rarely with the use of human albumin solutions, are flush, urticaria, fever, and nausea.
These reactions normally disappear rapidly when the infusion rate is slowed down or the infusion is stopped.
For safety information with respect to transmissible agents, see Precautions.
Tabulated list of adverse reactions: The table presented as follows is according to the MedDRA System Organ Classification (SOC) and Preferred Term Level (PT) and it includes undesirable effects occurring with the use of human albumin solutions.
Frequencies have been evaluated according to the following convention: very common (≥1/10); common (≥1/100 to <1/10); uncommon (≥1/1,000 to <1/100); rare (≥1/10,000 to <1/1,000); very rare (<1/10,000), not known (cannot be estimated from the available data).
There are no robust data on the frequency of undesirable effects from clinical trials.
The following data is in line with the safety profile of human albumin solutions, and confirmed by the post marketing experience; as the post marketing reporting of adverse reactions is voluntary and from a population of uncertain size, it is not possible to reliably estimate the frequency of these reactions: See Table 2.
 Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Paediatric population: No specific data are available on paediatric population.
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions via the national reporting system.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image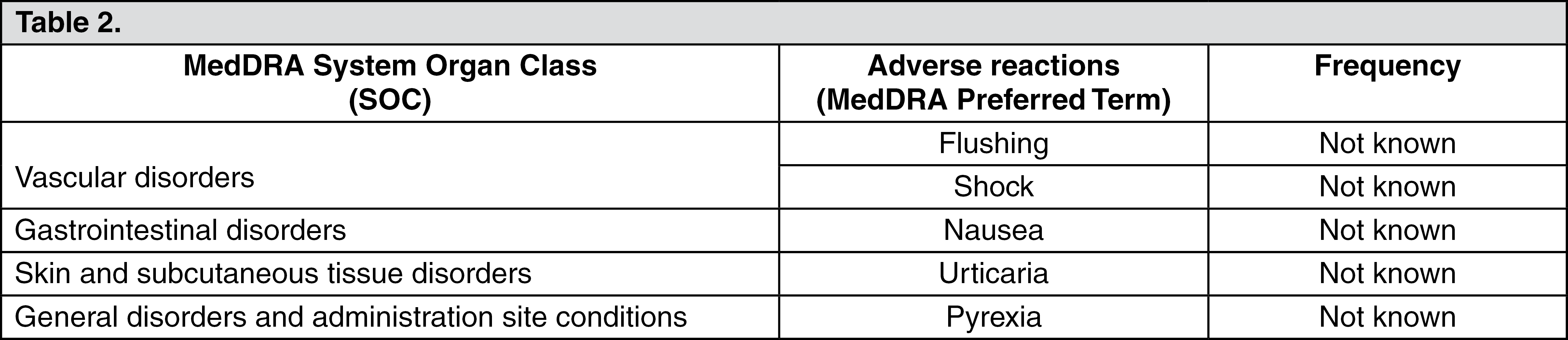 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
